In 2017, a baby girl was born in the USA as a result of a successful frozen-thawed transfer of an embryo that had been frozen for more than 25 years. This birth was indeed a milestone as it marked the first time in history that a successful pregnancy had resulted, after the transfer of an embryo that had been frozen for that long a time.
Since the first baby from a frozen embryo was born in 1984, embryo cryopreservation has been part of routine procedure in human assisted reproduction, where embryos are preserved by freezing them at sub-zero temperatures during the pre-implantation stages.
How does IVF work?
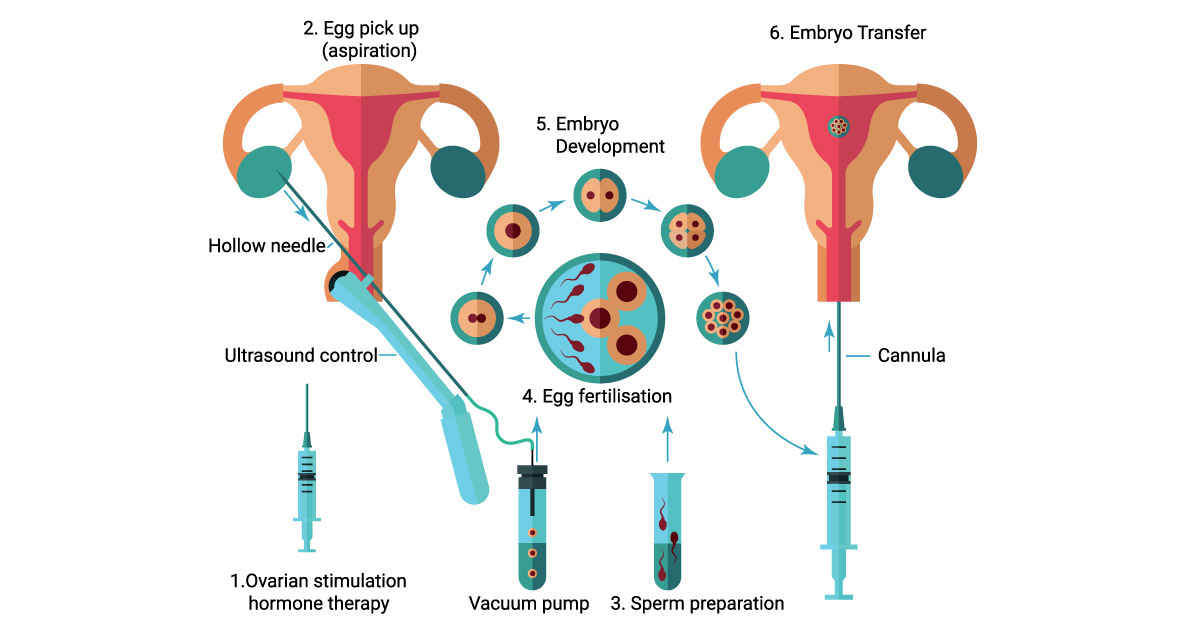
Why freeze embryos?
There are many circumstances where embryos are frozen. Sometimes, at the end of an In Vitro Fertilisation (IVF) cycle, an embryo transfer is not suitable because the lining of the womb (endometrium) is affected by the high level of hormones due to ovarian stimulation. Under these circumstances, embryos will first need to be frozen and only transferred later, when the patient’s womb environment has stabilised and become more suitable for conception. Another common situation that requires embryo freezing is when there are extra embryos available at the end of a fresh cycle. As only one (or a maximum of two) embryo are usually transferred at a time, the extra embryos are frozen for possible future use, in case the initial transfer is not successful.
At present, it is also possible to test embryos for genetic abnormalities prior to having the embryo transferred. This is called pre-implantation genetic testing (PGT). PGT involves taking a few cells from the embryo (usually a Day 5 or 6 embryo, called a blastocyst) and subjecting these cells to special genetic tests. As there may be a lag time between testing these cells and obtaining the results, these embryos will likely need to be frozen while awaiting the results.
Freezing eggs
Women can also opt to freeze their unfertilised eggs instead of embryos. Oocyte (egg) cryopreservation gives women reproductive autonomy since no male partner is needed, unlike in embryo freezing. It is suitable for women who are delaying their pregnancy for personal reasons like career advancement, or for young patients who are about to undergo treatment (such as chemotherapy or radiotherapy) which may affect their fertility. Freezing eggs is also a simpler choice to avoid ethical and legal complications in the future.
Cryopreservation methods
The main risks in cryopreservation are the formation of ice crystals inside and outside the cells and the dehydration of cells, which can damage them. Two methods of cryopreservation have been developed to solve these problems: slow programmable freezing and vitrification. Both methods involved the addition of cryoprotectants to protect cells from the effects of freezing. Today, vitrification is the preferred method by fertility centres for cryopreservation as it is faster, more efficient, and economical. More importantly, with vitrification, the risk of damage to embryos is reduced and the chance of survival after thaw is much improved. The advent of vitrification has led to frozen-thawed cycles having a better pregnancy rate compared to fresh transfer cycles, as well as a major shift towards blastocyst transfer.
Frequently asked questions
Q: How long can frozen embryos be stored?
A: The longest period an embryo has been frozen before resulting in a live birth is 25 years. Theoretically, it could last much longer, if stored properly. However, from a legal perspective, we are only allowed to keep frozen embryos for a period of 5 years in Malaysia, and possibly a further 5 years with approval from the Ministry of Health.
Q: Is there any difference of outcome between fresh and frozen embryo transfer?
A: In the past, fresh transfer pregnancy rates were consistently higher than frozen-thawed cycles. However, since the introduction of vitrification, frozen-thawed cycles have been exhibiting higher pregnancy rates compared to fresh cycles. By avoiding a fresh cycle transfer, the hormonal environment within the endometrial cavity is allowed to normalise before embryo transfer. Furthermore, a delayed transfer allows the selection of the best embryo for transfer, in contrast to selecting whichever embryo is available as often done in a fresh cycle.
Q: What are the approximate costs for embryo freezing?
A: The costs may differ from centre to centre depending on the facilities and expertise available. The approximate package cost for a fresh cycle excluding embryo transfer would be between RM16,000 to RM18,000. The frozen embryo transfer package would subsequently cost an additional RM3,500 to RM5,000, while an annual embryo storage fee is around RM1,000 to RM1,200.
Couples who are planning for fertility treatment can consider embryo freezing as part of their plan. The wife will not need to undergo multiple IVF cycles, which may be costly and painful, if the first transfer does not succeed. Couples going for treatment have to be prepared financially and mentally, as they might need several attempts before a successful pregnancy. As often said, fertility treatment can be an emotional, financial and logistics roller coaster!
An educational collaboration with Obstetrical and Gynaecological Society of Malaysia.





Comments